


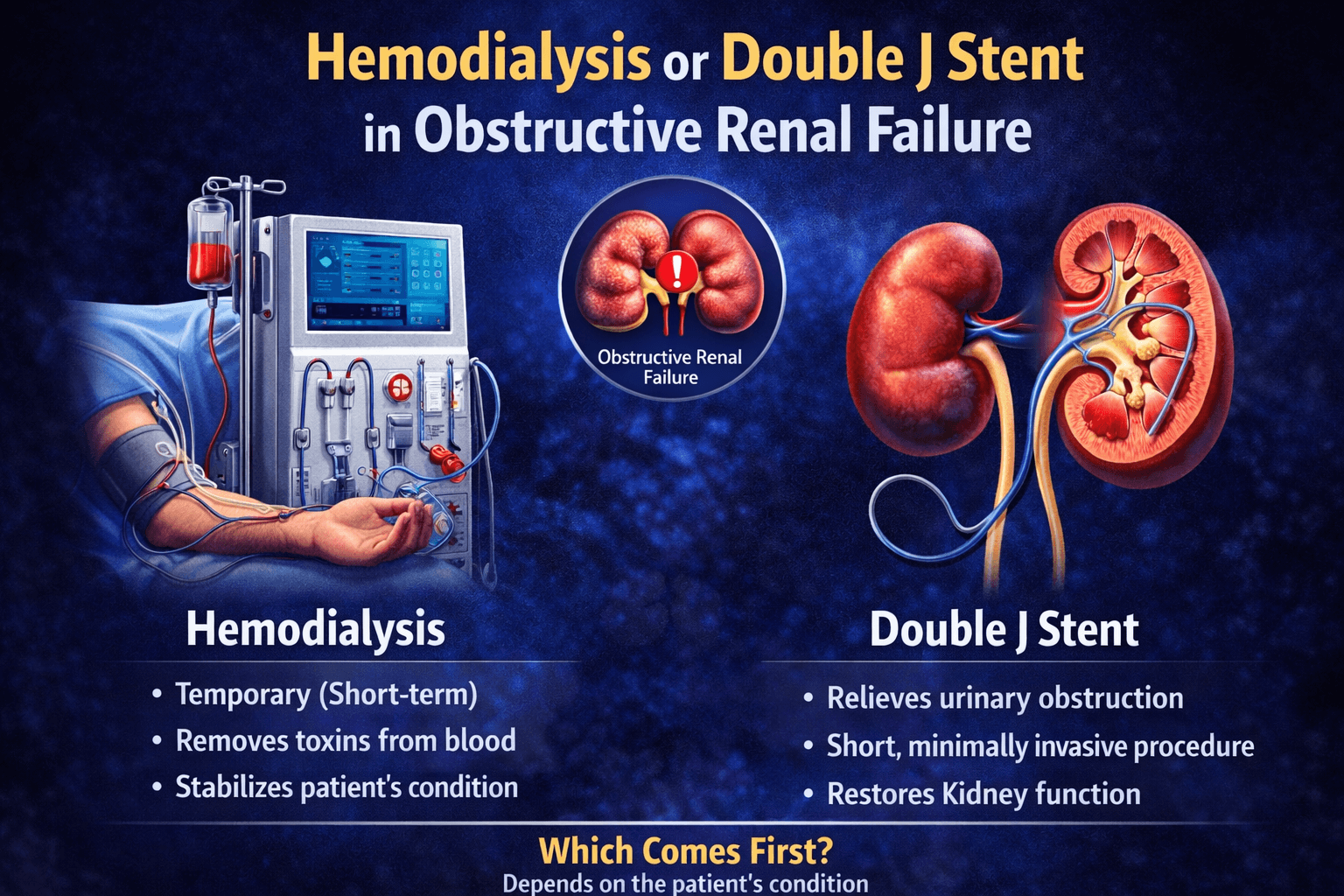
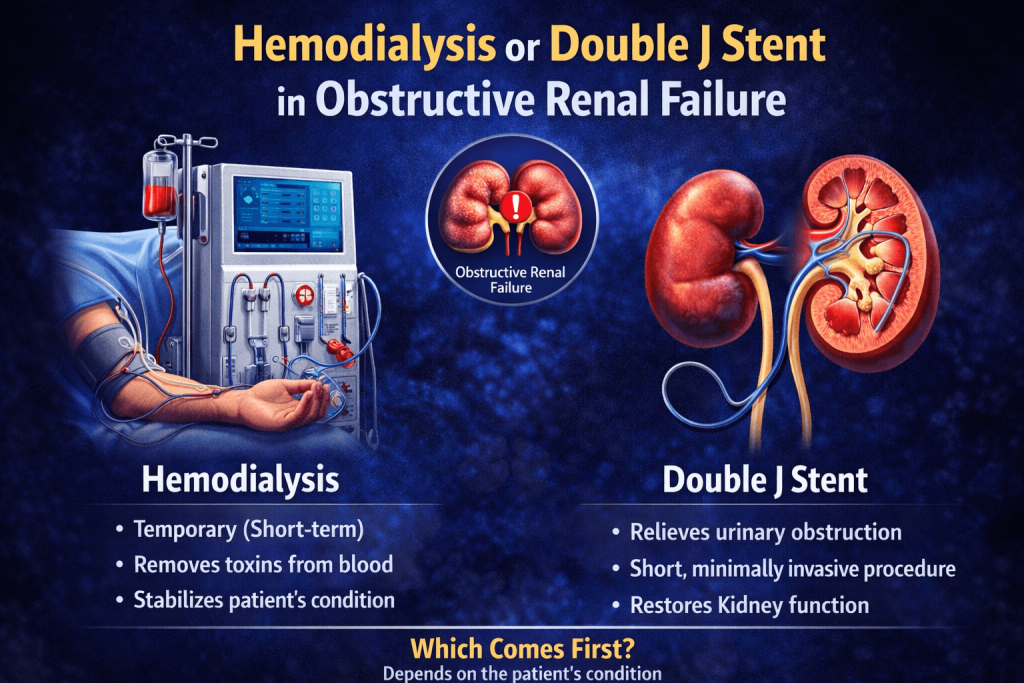
Obstructive renal failure, also known as obstructive uropathy, is a serious medical condition that occurs when the flow of urine is blocked, causing kidney dysfunction. This blockage can lead to acute kidney injury and requires prompt intervention to preserve renal function. Two critical treatment approaches for managing obstructive renal failure are hemodialysis and double J stent placement. Understanding when and how these interventions are used can help patients and healthcare providers make informed decisions about managing this potentially life-threatening condition.
Understanding Obstructive Renal Failure
Obstructive renal failure develops when an obstruction prevents urine from flowing normally through the urinary tract. This blockage causes pressure to build up in the kidneys, leading to kidney damage and impaired function. The obstruction can occur at any level of the urinary system, from the renal pelvis to the urethra.
Common causes of urinary tract obstruction include kidney stones, benign prostatic hyperplasia, tumors affecting the urinary tract, strictures, blood clots, and retroperitoneal fibrosis. The severity and duration of the obstruction determine the extent of kidney damage, making early diagnosis and treatment essential for optimal outcomes.
Symptoms of obstructive renal failure may include decreased urine output, flank pain, abdominal swelling, nausea, vomiting, and signs of uremia such as confusion and fatigue. Laboratory findings typically reveal elevated creatinine and blood urea nitrogen levels, indicating compromised kidney function.
Diagnosis of Obstructive Renal Failure
Accurate and timely diagnosis of obstructive renal failure is crucial for preventing irreversible kidney damage. The diagnostic process involves a combination of clinical evaluation, laboratory tests, and imaging studies to identify the location and cause of the obstruction.
Clinical Assessment
The diagnostic journey begins with a thorough medical history and physical examination. Physicians assess symptoms such as changes in urinary patterns, flank or abdominal pain, fever, and signs of fluid retention. A detailed history helps identify risk factors, including previous kidney stones, urinary tract infections, prostate problems, or pelvic malignancies.
Physical examination may reveal tenderness in the flank area, a distended bladder, or signs of fluid overload. In men, a digital rectal examination can detect prostate enlargement that might be causing lower urinary tract obstruction.
Laboratory Investigations
Blood tests are essential for evaluating kidney function and identifying metabolic complications. Key laboratory parameters include serum creatinine and blood urea nitrogen, which are typically elevated in renal failure. Electrolyte panels reveal potentially dangerous imbalances such as hyperkalemia, which can cause life-threatening cardiac arrhythmias.
Complete blood count may show anemia or elevated white blood cells, suggesting infection. Urinalysis can detect blood, infection, or crystals that provide clues about the underlying cause. In cases where infection is suspected, urine culture helps identify the causative organism and guide antibiotic therapy.
Imaging Studies
Imaging is the cornerstone of diagnosing obstructive renal failure, as it visualizes the urinary tract anatomy and identifies the site and cause of obstruction.
Renal Ultrasound is often the first-line imaging modality because it is non-invasive, readily available, and does not require contrast agents or radiation exposure. Ultrasound can detect hydronephrosis, which is the dilation of the renal collecting system due to urine backup. It can also identify kidney stones, masses, and bladder abnormalities.
CT Scan provides more detailed anatomical information and is considered the gold standard for diagnosing urinary tract obstruction. Non-contrast CT is particularly effective for detecting kidney stones, while contrast-enhanced CT can reveal tumors, vascular abnormalities, and the extent of hydronephrosis. CT urography offers comprehensive evaluation of the entire urinary tract.
Intravenous Pyelography (IVP) involves injecting contrast dye and taking X-ray images as it passes through the kidneys and urinary tract. While less commonly used today due to CT availability, IVP can provide functional information about kidney excretion.
MRI may be used in patients who cannot receive radiation or iodinated contrast, such as pregnant women. MR urography provides detailed anatomical images without radiation exposure.
Nuclear Renal Scan assesses kidney function and drainage, helping determine the degree of obstruction and whether kidney function is recoverable.
Indications for Treatment
Treatment decisions in obstructive renal failure depend on several factors, including the severity of kidney dysfunction, the location and cause of obstruction, the presence of infection, and overall patient health status.
Indications for Urgent Intervention
Certain clinical scenarios require immediate intervention to prevent permanent kidney damage or life-threatening complications:
Complete bilateral obstruction or obstruction in a patient with a solitary kidney represents a urological emergency requiring urgent decompression within hours to prevent irreversible renal damage.
Obstructive pyelonephritis occurs when a urinary tract infection develops above an obstruction, creating a closed-space infection that can rapidly progress to sepsis. This condition requires emergency drainage along with intravenous antibiotics.
Acute kidney injury with dangerous metabolic complications, including severe hyperkalemia, metabolic acidosis, or fluid overload, necessitates both relief of obstruction and possible hemodialysis.
Intractable pain from acute obstruction, particularly from kidney stones, may require urgent intervention for symptom relief even if kidney function is preserved.
Indications for Elective Management
Not all obstructive uropathy requires emergency treatment. Some situations allow for scheduled intervention:
Partial unilateral obstruction with preserved contralateral kidney function may be managed less urgently, allowing time for optimization and treatment planning.
Chronic partial obstruction causing progressive hydronephrosis but stable kidney function may require elective surgical correction of the underlying cause.
Small non-obstructing stones that are likely to pass spontaneously can be managed conservatively with pain control, hydration, and medical expulsive therapy.
Best Treatment Options for Obstructive Renal Failure
Treatment of obstructive renal failure aims to relieve the obstruction, preserve kidney function, manage complications, and address the underlying cause. The optimal approach depends on the location and severity of obstruction, patient factors, and available expertise.
Conservative Management
For partial obstruction without severe kidney dysfunction, conservative measures may be appropriate. This includes adequate hydration to promote urine flow, pain management with analgesics, medical expulsive therapy using alpha-blockers for distal ureteral stones, and close monitoring of kidney function and symptoms.
Patients with urinary tract infections require appropriate antibiotic therapy, though definitive obstruction relief is necessary for infection resolution in complete obstruction.
Double J Stent Placement
As discussed earlier, double J stent insertion is often the first-line intervention for relieving ureteral obstruction. The stent provides internal drainage, allowing urine to bypass the obstruction while maintaining kidney function.
Advantages of stent placement include being minimally invasive with quick recovery, allowing patients to remain ambulatory, providing immediate relief of obstruction, and enabling time for definitive treatment planning. Stents can remain in place for months, making them suitable for patients requiring neoadjuvant chemotherapy or radiation before definitive tumor surgery.
Limitations include urinary symptoms that can affect quality of life, risk of infection or encrustation with prolonged placement, and the need for eventual removal or exchange. Stents may not be possible in severe obstruction where the ureter cannot be accessed.
Percutaneous Nephrostomy
When retrograde stent placement is not feasible, percutaneous nephrostomy offers an alternative drainage method. This involves placing a catheter directly into the kidney through the skin under imaging guidance.
Indications for nephrostomy include failed retrograde stent placement, severe ureteral obstruction preventing stent passage, need for urgent drainage in an unstable patient, and situations where external drainage is preferred such as treating pyonephrosis.
Advantages include a high success rate even in complete obstruction, the ability to perform under local anesthesia, immediate pressure relief, and the option to convert to internal stenting later. The nephrostomy also allows access for antegrade stent placement or percutaneous stone removal procedures.
Disadvantages include requiring an external drainage bag, a higher risk of dislodgement compared to internal stents, more discomfort and lifestyle impact, and increased infection risk with prolonged use.
Hemodialysis
Hemodialysis serves as critical supportive therapy when kidney function deteriorates to dangerous levels. As previously detailed, hemodialysis manages life-threatening metabolic complications while allowing time for obstruction relief and kidney recovery.
The decision to initiate dialysis is based on clinical and laboratory criteria rather than creatinine levels alone. Patients with severe symptoms of uremia, refractory fluid overload, or dangerous electrolyte abnormalities require dialysis regardless of creatinine level.
Most patients with obstructive renal failure who require dialysis can discontinue it once the obstruction is relieved and kidney function recovers, though recovery may take days to weeks. Close monitoring with serial laboratory tests guides the decision to stop dialysis.
Definitive Surgical Treatment
While stents and nephrostomy tubes relieve obstruction temporarily, definitive treatment addresses the underlying cause:
Ureteroscopy with stone removal treats ureteral stones using minimally invasive endoscopic techniques. Laser lithotripsy fragments stones for extraction or spontaneous passage.
Extracorporeal shock wave lithotripsy (ESWL) uses focused shock waves to break kidney or ureteral stones into smaller pieces that can pass naturally.
Percutaneous nephrolithotomy (PCNL) removes large kidney stones through a small incision in the back, ideal for stones exceeding two centimeters.
Transurethral resection of the prostate (TURP) or laser prostate surgery relieves obstruction from benign prostatic hyperplasia.
Reconstructive surgery repairs ureteral strictures through ureteroureterostomy, ureteroneocystostomy, or other techniques depending on stricture location and length.
Tumor resection or debulking procedures, often combined with chemotherapy or radiation, treat malignant obstruction. Palliative stenting may be necessary for inoperable tumors.
Emerging and Advanced Treatment Options
Recent advances have expanded treatment options for complex cases:
Metallic ureteral stents offer longer durability for patients requiring prolonged stenting due to malignancy or complex strictures. These stents can remain in place for up to a year compared to three to six months for standard polymer stents.
Drug-eluting stents coated with medications that reduce inflammation and prevent tissue overgrowth are being investigated to improve patient comfort and extend stent life.
Robot-assisted surgery enables precise reconstructive procedures for complex ureteral injuries or strictures with improved outcomes and faster recovery.
Minimally invasive glue techniques for treating ureteral injuries show promise in selected cases, avoiding major surgery.
Choosing the Right Treatment Approach
Selecting the optimal treatment requires individualized assessment considering multiple factors:
Obstruction characteristics, including location, degree of obstruction, unilateral versus bilateral involvement, and underlying cause, guide initial management decisions.
Kidney function status determines urgency and whether dialysis support is needed alongside obstruction relief.
Patient factors such as overall health, ability to tolerate procedures, presence of infection, and personal preferences influence treatment selection.
Local expertise and resources affect which procedures can be performed safely and effectively at a given institution.
Long-term considerations including the need for cancer treatment, likelihood of obstruction recurrence, and patient lifestyle impact, should factor into treatment planning.
The Role of Double J Stent in Treating Obstruction
A double J stent, also called a ureteral stent or JJ stent, is a thin, flexible tube inserted into the ureter to maintain urine flow from the kidney to the bladder. The stent features curl-shaped ends resembling the letter “J” at both terminals, which prevents migration and keeps the device properly positioned.
The Stent Placement Procedure
Double J stent insertion is typically performed as a minimally invasive procedure under local anesthesia with sedation or general anesthesia. Using cystoscopy, the urologist visualizes the bladder and ureteral opening, then guides the stent through the ureter into the renal pelvis using fluoroscopic guidance.
The procedure usually takes thirty to sixty minutes and can often be done as an outpatient procedure or with a short hospital stay. In cases where retrograde stent placement is not possible due to severe obstruction or anatomical challenges, an antegrade approach through percutaneous nephrostomy may be necessary.
Benefits and Outcomes
The primary advantage of double J stent placement is rapid decompression of the obstructed kidney, which can prevent irreversible damage to renal tissue. Studies show that early stent placement significantly improves renal function recovery, with many patients experiencing substantial creatinine reduction within days to weeks of the procedure.
The stent remains in place for weeks to months, depending on the underlying cause of obstruction and whether definitive treatment is planned. During this time, patients can maintain relatively normal kidney function while addressing the root cause of the obstruction, whether through stone removal, tumor treatment, or surgical correction.
Potential Complications
While generally safe, double J stent placement can cause complications, including lower urinary tract symptoms such as urinary frequency, urgency, and discomfort during urination. Some patients experience hematuria, stent migration, infection, or encrustation requiring stent replacement. Regular follow-up and timely stent removal or exchange are essential to prevent these complications.
Hemodialysis in Obstructive Renal Failure
Hemodialysis is a renal replacement therapy that filters waste products, excess fluid, and toxins from the blood when the kidneys cannot adequately perform this function. In obstructive renal failure, hemodialysis serves as a temporary life-saving measure when kidney function deteriorates to dangerous levels.
When Is Hemodialysis Required?
Not all patients with obstructive renal failure require hemodialysis. The decision to initiate dialysis depends on the severity of kidney dysfunction and the presence of life-threatening complications. Specific indications for emergency hemodialysis include severe hyperkalemia with cardiac arrhythmia risk, severe metabolic acidosis, fluid overload causing pulmonary edema, and uremic symptoms such as pericarditis or altered mental status.
Hemodialysis is typically indicated when conservative management and stent placement alone cannot adequately address the metabolic derangements caused by acute kidney injury. The goal is to stabilize the patient while allowing time for the stent or nephrostomy to relieve the obstruction and permit kidney function recovery.
How Hemodialysis Works
During hemodialysis, blood is removed from the body through vascular access, passed through a dialyzer or artificial kidney that filters waste and excess fluid, and then returned to the body. The process typically requires three to four hours per session and may be needed daily or several times weekly depending on the severity of kidney dysfunction.
For acute situations, temporary vascular access is established through a central venous catheter placed in the jugular, femoral, or subclavian vein. This allows immediate initiation of dialysis without waiting for the creation of permanent access like an arteriovenous fistula.
The Complementary Approach
In obstructive renal failure, hemodialysis and double J stent placement often work together rather than as competing treatments. The stent addresses the underlying obstruction and allows kidney recovery, while hemodialysis manages the immediate metabolic consequences of kidney failure until function improves.
Many patients with severe obstructive renal failure initially require both interventions. After stent placement relieves the obstruction, serial monitoring of kidney function helps determine when dialysis can be safely discontinued. The majority of patients with reversible obstruction can eventually discontinue dialysis as their kidney function recovers, though recovery time varies depending on obstruction duration and severity of initial kidney injury.
Recovery and Prognosis
The prognosis for patients with obstructive renal failure depends heavily on the timing of intervention. When obstruction is relieved within days to weeks, most patients experience substantial kidney function recovery. However, prolonged obstruction lasting months can cause irreversible kidney damage requiring permanent dialysis.
Studies indicate that bilateral obstruction or obstruction in a solitary kidney carries higher risk for permanent kidney damage compared to unilateral obstruction with a functioning contralateral kidney. Age, underlying comorbidities, and the cause of obstruction also influence outcomes.
After stent placement, patients require regular follow-up with imaging studies and laboratory tests to monitor kidney function recovery and ensure the stent remains properly positioned. Once the underlying cause is definitively treated, the stent can be removed, though some conditions may require long-term stenting with periodic exchanges.
Prevention and Long-Term Management
Preventing obstructive renal failure involves managing risk factors and underlying conditions. Patients with recurrent kidney stones benefit from dietary modifications, adequate hydration, and sometimes medications to prevent stone formation. Men with benign prostatic hyperplasia should receive appropriate treatment to prevent urinary retention and upper tract obstruction.
Regular monitoring is essential for patients at high risk for obstruction, including those with pelvic malignancies, retroperitoneal tumors, or recurrent urolithiasis. Early detection and intervention can prevent severe kidney injury and reduce the need for dialysis.
Lifestyle modifications play an important role in prevention. Maintaining adequate fluid intake, typically eight to ten glasses of water daily, helps prevent stone formation and maintains good urinary flow. Limiting sodium intake reduces calcium excretion in urine, decreasing stone risk. For patients with recurrent stones, specific dietary restrictions based on stone composition analysis may be recommended.
Conclusion
Both hemodialysis and double J stent placement play vital roles in managing obstructive renal failure, serving different but complementary purposes. The double J stent directly addresses the obstruction by restoring urine drainage and allowing kidney recovery, while hemodialysis provides critical metabolic support when kidney function is severely compromised.
Prompt recognition of obstructive renal failure and timely intervention with stent placement offers the best chance for kidney function recovery and avoiding permanent dialysis dependence. The key to successful outcomes lies in accurate diagnosis using appropriate imaging studies, understanding the indications for different treatment modalities, and selecting the best treatment option based on individual patient characteristics.
Working closely with nephrologists and urologists ensures comprehensive care that addresses both the immediate life-threatening complications and the underlying cause of obstruction. With appropriate treatment, many patients achieve substantial or complete recovery of kidney function, highlighting the importance of early diagnosis and intervention in this potentially reversible form of kidney failure.
For patients in Multan seeking expert urological care for obstructive renal failure, Dr. Abdul Ghaffar is recognized as one of the best urologists in Multan. With extensive experience in advanced urological procedures, including double J stent placement, percutaneous nephrostomy, and comprehensive management of kidney-related conditions, Dr. Abdul Ghaffar provides professional treatment options tailored to each patient’s specific needs. Consulting with an experienced specialist like Dr. Abdul Ghaffar can ensure you receive an accurate diagnosis, appropriate treatment selection, and optimal outcomes for your urological condition.

{kind=link}